
Vesicoureteral Reflux
What is vesicoureteral reflux?
Normally, urine flows from the kidneys down the ureters into the bladder then out through the urethra. Vesicoureteral reflux (VUR) is a pediatric condition most frequently diagnosed in infancy and childhood. When a child has VUR, urine flows backward—from the bladder to the kidneys – through one or both ureters. Children born with VUR lack the valve function that prevents urine from flowing back from the bladder up to the kidneys. VUR on its own is not necessarily dangerous.
Children with VUR who develop a urinary tract infection are at risk of the infection traveling to the kidney and causing pyelonephritits. These infections may then cause scarring and damage to the kidneys. Over time, increased scarring and damage to kidneys can cause decreased kidney function and high blood pressure. It is important to understand, however, that reflux does not cause urinary tract infections and urinary tract infections do not cause reflux. Learn more about urinary tract infections.

What causes vesicoureteral reflux?
The cause of VUR is not fully understood. Some studies have shown there to be a higher chance of a child having VUR if their parents or siblings have a history of VUR. Also, having other urinary tract abnormalities, such as ureterocele, ureter duplication or posterior urethral vales increases the risk of having VUR.
The cause of VUR is usually mechanical. Children may have a faulty valve where the ureter enters into the bladder or ureters that enter the bladder at an abnormal position. Other children may have a blockage in the urethra that does not allow urine to pass easily out of the body, thus increasing the pressure in the bladder and causing urine to flow back up the ureter.
What are the symptoms of vesicoureteral reflux?
There are no specific symptoms of VUR. However, frequent and recurrent urinary tract infections with fevers (called a febrile UTIs) in children might be a symptom of VUR. In fact, VUR is present in nearly one-third of children who have a febrile UTI. It is important to understand, however, that reflux does not cause urinary tract infections and urinary tract infections do not cause reflux. Signs of a urinary tract infection may include:
- Foul smelling or cloudy urine
- Fever
- Stomach ache
- Backache
- Side pain
- Burning or pain while urinating
- Frequent and urgent urination
- Headache
- Vomiting
Because the symptoms of VUR may resemble other conditions or medical problems, it is best to speak with one of the pediatric urology specialists at the CHOC Urology Center.
How is vesicoureteral reflux diagnosed?
VUR is usually first diagnosed in a child after an episode of pyelonepritis. If there is a family history of VUR, but a child has no symptoms, the child’s physician may elect to perform a diagnostic test to rule out VUR. Diagnostic procedures for VUR may include:
- Voiding cystourethrogram (VCUG). This allows for direct imaging of a refluxing ureter. A VCUG is a specific X-ray that examines the urinary tract. A catheter (hollow tube) is placed in the urethra (tube that drains urine from the bladder to the outside of the body) and the bladder is filled with a liquid dye. X-ray images are taken as the bladder fills and empties. The images show if there is reverse flow of urine into the ureters and/or kidneys. VCUGs are a common procedure, but children and parents often find the catheter to be unpleasant. Sometimes a numbing gel is used to help ease discomfort. Talking to your child before the procedure, so they are aware of what to expect can help ease anxiety. Additionally, the more relaxed the child is during the procedure the less discomfort they will feel.
- Renal ultrasound. This will not identify reflux but will provide vital information about the kidneys that will be used in generating a treatment plan. This is a noninvasive test in which a transducer is passed over the kidney producing sound waves which bounce off the kidney, transmitting a picture of the organ on a video screen. The test is used to determine the size and shape of the kidney and to detect a mass, kidney stone, cyst or other obstruction or abnormalities. (Most parents are familiar with ultrasounds from during pregnancy.)
Learn more about the common diagnostic procedures used at the CHOC Urology Center.
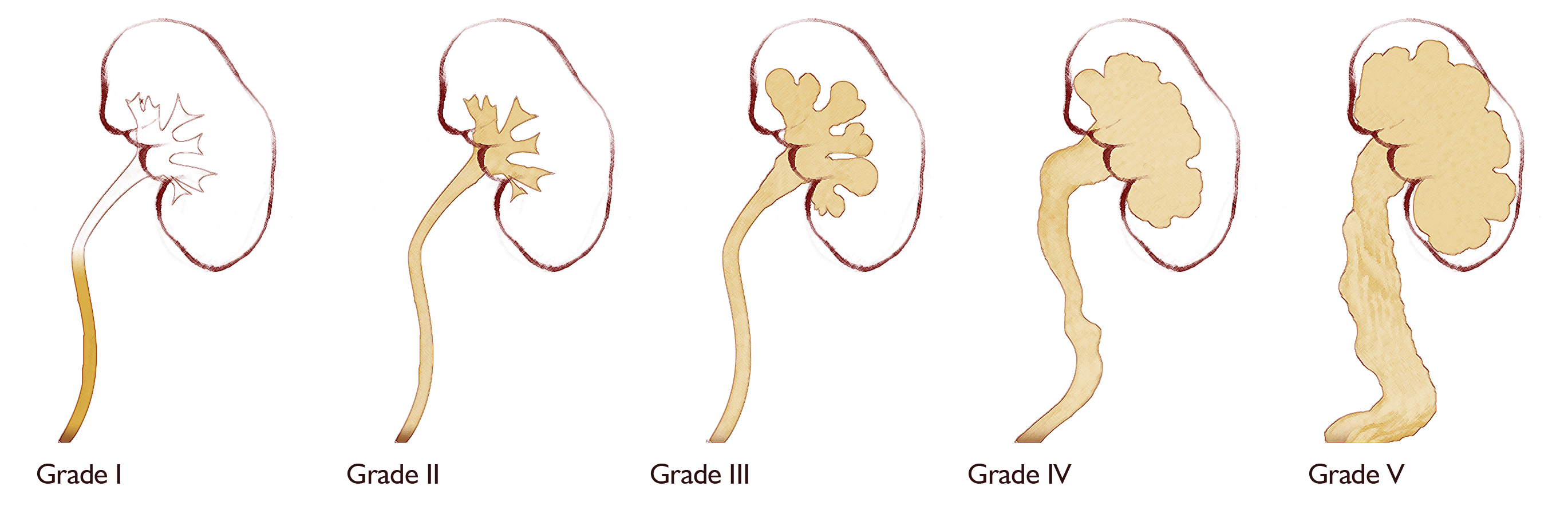
How is VUR graded?
VUR is graded according to the images obtained on a VCUG. The lower the grade of reflux the higher the chances are that it will resolve without surgery. It is possible to have VUR bilaterally (on both sides) and that the grades will be different.
- Grade 1: This is the mildest form of VUR. The ureters appear normal in size and urine flows up into the ureter but not into the kidney.
- Grade 2: Urine travels all the way up the ureter and enters the part of the kidney where urine is collected before draining (renal pelvis). The ureter is normal in size.
- Grade 3: Similar to grade 2 expect that the ureters and/or the renal pelvis look more full.
- Grade 4: Similar to grade 3 except that the ureter is grossly enlarged and the calyces of the kidney are more blunted.
- Grade 5: Most severe state of VUR. Similar to grade 4 plus the ureter is very full and tortuous (full of twists).
What is the treatment for vesicoureteral reflux?
Our specialists work with each patient and the patient’s family to determine the best course of treatment based on:
- The child’s age, overall health and medical history.
- The extent of the condition.
- The child’s tolerance for specific medications, procedures or therapies.
- Expectations for the course of the condition.
- The family’s preferences.
Our specialists may assign a grading system (ranging from 1 to 5) to indicate the degree of the child’s. The higher the grade, the more severe the reflux.
Many cases of reflux, especially those with a lower grade, can resolve over time, usually within five years. At CHOC, we believe in trying to reduce the chances of a child having recurrent urinary tract infections, which cause VUR complications. Most children will be recommended to start on prophylactic antibiotics until they are toilet trained to help keep their urine sterile and free of bacteria. This treatment option allows us to protect the child from urinary tract infections while waiting for the VUR to go away by itself. Some parents are concerned about the long-term use of antibiotic prophylaxis due to the risk of antibiotic resistance — a condition in which bacteria become resistant to the low dose of antibiotics over time so that the antibiotics are no longer effective on the child. With proper dosing an antibiotic has a minimal effect on antibiotic resistance.
When children are toilet trained we work with the child and family to ensure that they are practicing the best behavioral modifications to reduce their chances of developing infections. Children are monitored with repeated ultrasounds as they grow to ensure there is no damage to the kidneys. The VCUG is not performed regularly but is often repeated when a child is school-aged or if they persist with complications such as breakthrough infections of recurrent febrile UTIs.
When an infection occurs while a child is on prophylactic antibiotics, it is referred to as a breakthrough infection. If a child persists with recurrent febrile UTIs (when not on prophylaxis) or breakthrough infections then they may require a surgical intervention to resolve their reflux. The common procedure completed is a cystoscopy and Deflux injection. Deflux is a gel made from two sugar-based materials that is injected into the refluxing ureter. The procedure is minimally invasive and does not require an incision.
Some children will not be good candidates for Deflux or the Deflux may fail. If this occurs a ureteral reimplant surgery can be completed at our facility. This surgery involves removing the ureter where it joins the bladder and reimplanting it at another spot on the bladder. It is about 99% effective in resolving reflux.
After any surgical intervention a repeated VCUG and ultrasound are completed to see if the VUR has resolved.