
Hydronephrosis
The specialists at the CHOC Urology Center work one-on-one with each patient to determine the cause of each child’s hydronephrosis in order to create a customized treatment plan.
What is hydronephrosis?
Hydronephrosis is a common congenital condition that is found in about one out of every 500 babies. In very rare cases, hydronephrosis can be developed later in life as well. Hydronephrosis is a treatable condition in which urine gets trapped in the kidney and drains slower than it should into the bladder. This causes the kidney to appear swollen. Hydronephrosis can affect one kidney (unilateral) or both kidneys (bilateral). It is often referred to as being ‘prenatal’ or ‘antenatal.’ The term prenatal means the hydronephrosis was noticed in the child before birth. Antenatal means the hydronephrosis was noted after birth.
Today, hydronephrosis is usually first diagnosed on prenatal ultrasounds. Finding hydronephrosis while the baby is the womb has become more common because of advances in prenatal ultrasounds. Before the advancement in this technology, children born with hydronephrosis may not have been diagnosed until they began to show symptoms, or were not identified at all. Many children who are diagnosed with hydronephrosis before they are born will have the condition resolve on its own while the child is young, without medical intervention.
What causes hydronephrosis?
A number of conditions can cause hydronephrosis. In some children, the root cause of the hydronephrosis may never be known.
While there can be many conditions that lead to hydronephrosis, the most common causes are obstructions (blockages) that reduce the ability of urine to flow out of the kidney and into the bladder. These obstructions can include:
- UPJ obstruction is a blockage at the point where the kidney meets the ureter (the tube that carries urine to the bladder).
- UVJ obstruction is a blockage at the point where the ureter (the tube that carries urine to the bladder) meets the bladder.
- Posterior urethral valves (PUV) are an obstruction that occurs prior to birth in males that is caused by pieces of tissue in the area of the prostatic urethra.
- Ureterocele occurs when the ureter does not develop properly and causes a small pouch into the bladder.
Other causes can be:
- Vesicoureteral reflux occurs when urine in the bladder flows back into the ureters and often back into the kidneys.
- Ectopic Ureter drains urine somewhere outside the bladder.
- Neurogenic Bladder is a condition in which the nerves that carry messages from the bladder to the brain and from the brain to the muscles of the bladder do not work properly.
For more information on the conditions above, we encourage families to read our guide to conditions treated at the CHOC Urology Center.
How is hydronephrosis diagnosed?
Hydronephrosis is most commonly diagnosed on routine prenatal ultrasounds completed after 10 weeks of gestation. Children diagnosed with hydronephrosis while in the womb or later in life often receive renal ultrasounds, Lasix renal scans and/or voiding cystourethrograms so that the urology team may gain a more complete understanding of the hydronephrosis and monitor the child’s condition. Please see our guide to common diagnostic procedures for complete information on these tests.
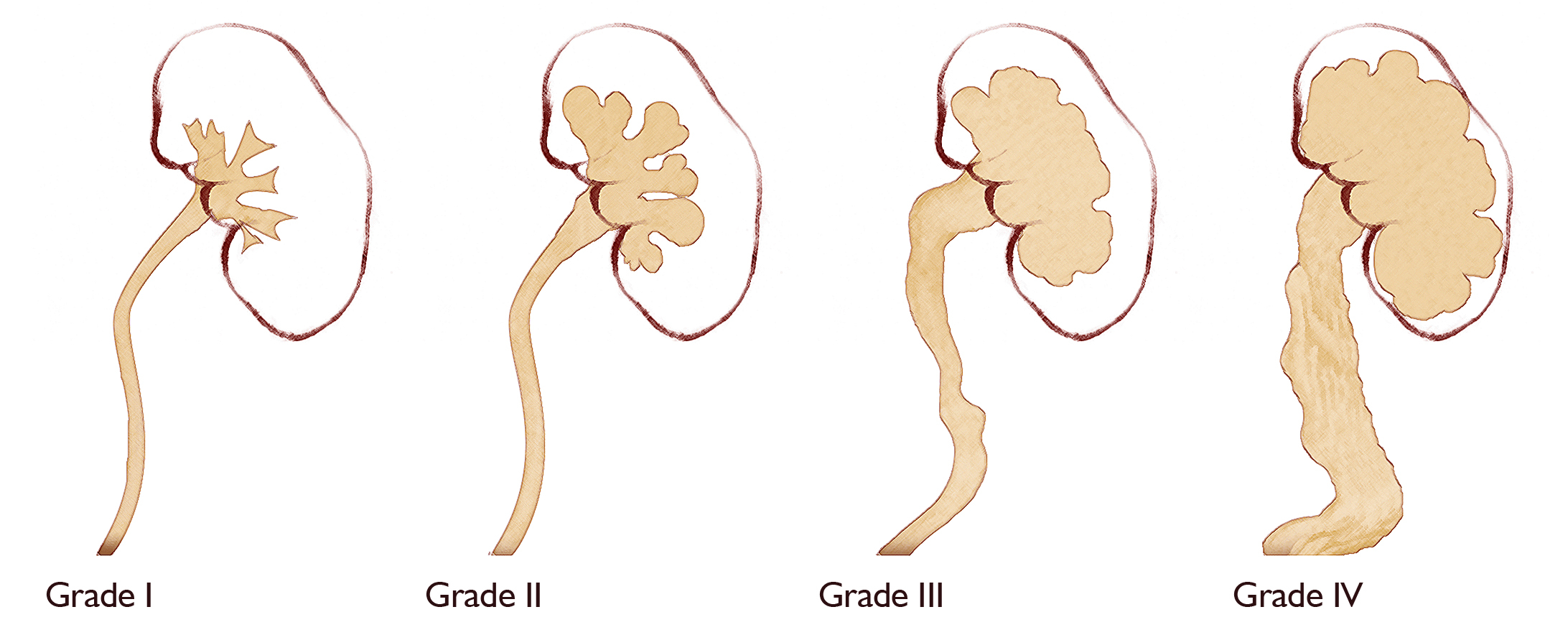
What is the grading system for severity of hydronephrosis?
Based on the child’s ultrasounds, a member of the CHOC Urology staff and a radiologist will determine the grading of the child’s hydronephrosis. The Society for Fetal Urology has created a universal grading system of hydronephrosis that ranges from grade 1 (most mild) to grade 5 (most severe). The grading system is based on how dilated the kidney and the amount of renal paranchemya present.
What are the signs and symptoms of hydronephrosis?
Most infants with hydronephrosis have no symptoms at all. Older children may also have no symptoms and the condition may disappear without intervention.
If a child has more severe hydronephrosis, they may experience one or more of the following symptoms:
- Abdominal pain with nausea and/or vomiting, especially after large fluid intakes.
- Flank pain (just above the hipbone slightly to the back).
- Hematuria (blood in their urine).
- Urinary tract infections
What is the treatment for hydronephrosis?
Hydronephrosis is monitored at the CHOC Urology Center with ultrasounds. Most children will have an ultrasound completed about once every three months during their first year of life in order for the degree of hydronpehoris and its progression to be properly determined. Many children diagnosed prenatally with hydronpehrosis will see their condition resolve without surgical intervention. Most cases of mild and moderate hydronephrosis only need periodic monitoring.
If a child’s hydronephrosis worsens over time or is severe, medical intervention may be necessary. If this is the case, a surgery may be carried out by one of our fellowship-trained pediatric urologists. The most common procedure completed to correct hydronephrosis is a pyeloplasty. During a pyeloplasty, the narrowed or obstructed part of the ureter is removed and the ureter is reconnected to the healthy portion of the kidney’s drainage system. The success rate of a pyeloplasty is about 95 percent. There are cases where other surgeries may be needed. Learn about postoperative care after pyeloplasty.
What are the long-term consequences of hydronephrosis?
Children with hydronephrosis typically lead normal lives, as most cases of the condition resolve early in their life, often without long-term consequence. Even children with hydronephrosis that does not quickly resolve typically have no kidney damage and will lead normal lives. In some cases, hydronpehrosis that is severe or left untreated may cause some degree of renal failure that may cause long-term complications for the child.