
Endoscopy
Call today to schedule an appointment with one of our pediatric specialists.
Gastroenterology Referrals
View the referral guidelines
What is an upper endoscopy?
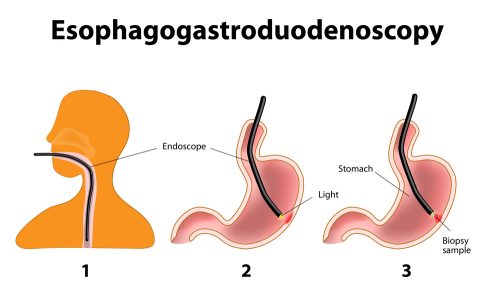
Upper endoscopy (also referred to as an EGD, esophagogastroduodenoscopy, upper gastrointestinal endoscopy, upper GI endoscopy, gastroscopy, esophagoscopy or endoscopy) is a procedure that allows a doctor to diagnose and treat problems in the upper gastrointestinal (UGI) tract.
Why would a child need an upper endoscopy?
An upper endoscopy may be performed to diagnose structural or functional problems of the esophagus, stomach and/or duodenum. These may include, but are not limited to, the following:
- Dysphagia (difficulty swallowing)
- Weight loss or anorexia (loss of appetite).
- Upper abdominal pain or chest pain that does not appear to be related to the child’s heart.
- Gastroesophageal reflux disease (GERD)
- Continuous vomiting from an unknown cause.
- To remove obstructions like food or coins in the esophagus.
- To better understand damage caused by the ingestion of substances like lye and household detergents.
- Suspected eosinophilic esophagitis or reassessment of the esophagus after food elimination or reintroduction.
Your child’s doctor may recommend an upper endoscopy procedure to:
- Evaluate symptoms: An upper endoscopy procedure will help your child’s doctor determine what is causing any symptoms related to digestion, including abdominal pain or discomfort, nausea, vomiting and difficulty swallowing.
- Make a diagnosis: Your child’s doctor will then analyze the results of the procedure in order to make a diagnosis. This may involve a biopsy, or tissue sampling, to test for any diseases or underlying conditions such as anemia, inflammation, diarrhea, bleeding or cancers of the digestive system.
- Establish a treatment plan: After a diagnosis is made, your child’s doctor will come up with a treatment plan to resolve any symptoms. During this step of the procedure, a special tool can be passed through the endoscope in order to treat any primary concerns, like stopping any bleeding from broken vessels, widening a narrow esophagus or removing any blockages.
How is an endoscopy performed?
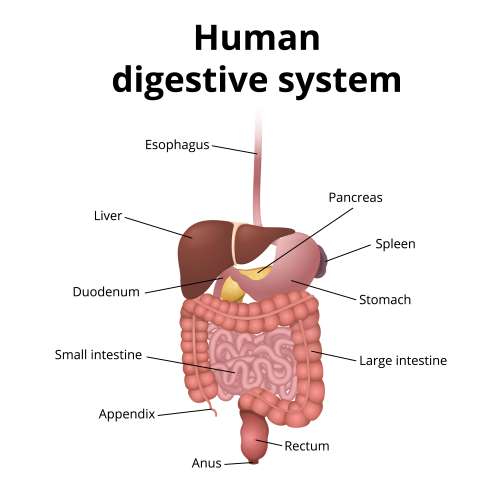
To perform the procedure, the doctor uses a long, flexible, lighted tube called an endoscope. The endoscope is guided through the patient’s mouth and throat, then through the esophagus, stomach and duodenum (first part of the small intestine). The physician can examine the inside of these organs and detect abnormalities. In addition to performing visual examination of the UGI tract with the endoscope, the doctor can insert instruments through the endoscope to get tissue samples for a biopsy, remove foreign objects, instill air or fluid, stop bleeding or perform therapeutic procedures, such as endoscopic surgery, laser therapy or dilatation (opening up). A video camera in the endoscope provides images onto a TV-like monitor.
What are the risks involved with endoscopy?
As with any procedure, complications can occur. Some possible risks may include, but are not limited to:
- Infection
- Bleeding
- Perforation (a tear in the lining) of the duodenum, esophagus or stomach.
How do I prepare my child for an endoscopy?
The child’s physician or nurse practitioner will explain the procedure during a clinic visit. This is a great time to ask questions; there are no questions that are too basic or silly to ask. During this visit, the child’s parent or legal guardian will be asked to sign a consent form that gives permission to do the test. It is important for caregivers to read the form carefully and ask questions if something is not clear.
Caregivers should notify the physician if the child is sensitive to or is allergic to any medications, latex, tape or anesthetic agents (local and general). The physician should also be told if the child has a history of bleeding problems or is taking any medications, including prescribed and over-the-counter medicines, as well as vitamins and herbal supplements. Learn more about how to prepare children of all ages for surgery.
Depending upon the child’s age, restrictions are placed on when the child can eat or drink prior to surgery. These guidelines are referred to as “NPO guidelines” and not following these guidelines as discussed may result in the procedure being delayed or rescheduled for another day. Learn more about the CHOC NPO guidelines.
What happens the day of an endoscopy?
All patients scheduled for a procedure should valet park and check-in in the hospital lobby two hours prior to the procedure. Once checked in, patients and their families are escorted to the preoperative unit where the child’s IV is started and staff, including child life specialists, help prepare the child for the procedure. Learn more about what to expect the day of surgery in our Day of Surgery Guide for Patients and Families.
When it is time for the actual procedure, the child is taken to the endoscopy suite. Family members are unable to be with the child during this time. However, the child will be carefully monitored by a board-certified anesthesiologist throughout the procedure using what is called “monitored anesthesia.” The child will breathe on their own, but will be in a deep sleep. The child’s blood pressure, heart rate, breathing rate, skin color and oxygen levels are constantly observed. The procedure itself takes about 10 minutes.
What happens if the doctor is taking a biopsy?
After the visual inspection of the esophagus, stomach and small bowel has been completed, the physician will take freckle-sized pieces of tissue from the lining of the small intestine, bowel, stomach and esophagus. These tissue samples are called biopsies. The staff in the endoscopy suite will prepare the pieces of tissue for examination under a microscope. This exam is done by a special physician called a pathologist. This is a very important part of the test as it will provide important information about the child’s condition.
What happens after an endoscopy procedure?
After the procedure, parents or legal guardians have an opportunity to speak with the physician to get their immediate feedback about the procedure and view some pictures taken during the upper endoscopy.
After a short time in recovery, the child will come back to the preoperative unit for observation. He or she will need to stay at the hospital until they are fully awake and able to take fluids without vomiting. Most children will go home the same day. Learn more about what to expect after the child’s procedure is complete and during discharge.
How should I care for my child at home after an endoscopy?
Most children can return to their normal activity after they have recovered from the sedation provided during the procedure. The child’s physician may provide additional or alternate instructions after the procedure, depending on the child’s particular situation.
When to call the doctor
It is important to notify the doctor if the child experiences any of the following after returning home:
- Fever and/or chills
- Redness, swelling, bleeding or other drainage from the IV site
- Abdominal pain, nausea and/or vomiting
- Black, tarry or bloody stools
- Swallowing difficulties
- Throat or chest pain that worsens or does not get better after 48 hours.