
Heart Valve Repair or Replacement
Call today to schedule an appointment with one of our pediatric specialists.
Cardiothoracic Surgery Referrals
Because families are bound to have many questions about heart valve repair or heart valve replacement, our pediatric cardiologists have developed answers to some of the most frequently asked questions about these surgeries. It is important to remember that this information is not intended to replace instructions provided by the child’s health care team.
What is heart valve repair or replacement surgery?
Heart valve repair or replacement surgery is a treatment option for valvular heart disease. When heart valves become damaged or diseased, they may not function properly. Conditions which may cause heart valve dysfunction are valvular stenosis and valvular insufficiency (regurgitation).
When one (or more) valve(s) becomes stenotic (stiff), the heart muscle must work harder to pump the blood through the valve. Some reasons why heart valves become stenotic include infection (such as rheumatic fever or staphylococcus infections) or congenital heart defects (structural heart problems). If one or more valves become insufficient (leaky), blood leaks backwards, which means that less blood is pumped in the proper direction. Based on the child’s symptoms and overall condition of their heart, the doctor may decide that the diseased valve(s) needs to be surgically repaired or replaced.
Traditionally, repair or replacement of heart valves has involved open-heart surgery, which means that the chest is opened in the operating room and the heart stopped for a time so that the surgeon may repair or replace the valve(s). In order to open the chest, the breastbone, or sternum, is cut in half and spread apart. Once the heart is exposed, large tubes are inserted into the heart so that the blood can be pumped through the body during the surgery by a cardiopulmonary bypass machine (heart-lung machine). The bypass machine is necessary to pump blood because the heart is stopped and kept still while the surgeon performs the valve repair or replacement procedure.
The diseased valve may be repaired using a ring to support a person’s own valve, or the entire valve may be removed and replaced by an artificial valve made out of plastic, metal or tissue.
Newer, less invasive techniques have been developed to replace or repair heart valves. Minimally invasive procedures make smaller incisions–and mean less pain afterward and shorter hospital stays. Balloon valvuloplasty is one such procedure. It’s used to treat some cases of valve stenosis, and is done as part of a catheterization procedure, rather than as part of open-heart surgery.
Other related procedures that may be used to assess the heart include:
- Resting and exercise electrocardiogram (ECG/EKG)
- Holter monitor
- Cardiac catheterization
- Chest X-ray
- Ultrafast computed tomography (CT scan) of the chest
- Echocardiograms
- Electrophysiological studies
- Magnetic resonance imaging (MRI) of the heart.
How do the valves of the heart work?
To better understand how valvular heart disease affects the heart, a review of basic heart anatomy and valve function follows.
The heart is a pump made of muscle tissue. The heart has four pumping chambers: two upper chambers, called atria, and two lower chambers, called ventricles. The right atrium pumps blood into the right ventricle, which then pumps the blood into the lungs where wastes such as carbon dioxide are given off and oxygen and other nutrients are taken into the blood.
From the lungs, the blood flows back into the left atrium, is pumped into the left ventricle, and then is pumped through the aorta out to the rest of the body and the coronary arteries. When the atria are contracting, the ventricles are relaxed in order to receive the blood from the atria. Once the blood from the atria has passed into the ventricles, the atria relax while the ventricles pump the blood out to the lungs and to the rest of the body.
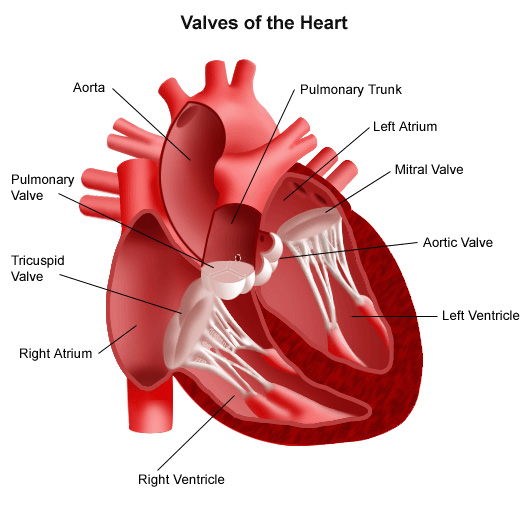
In order to keep the blood flowing forward during its journey through the heart, there are valves between each of the heart’s pumping chambers:
- Tricuspid valve. Located between the right atrium and the right ventricle.
- Pulmonary (or pulmonic) valve. Located between the right ventricle and the pulmonary artery.
- Mitral valve. Located between the left atrium and the left ventricle.
- Aortic valve. Located between the left ventricle and the aorta.
If the heart valve(s) becomes damaged or diseased, a person may experience the following symptoms:
- Dizziness
- Chest pain
- Breathing difficulties
- Difficulty keeping up with peers while playing
- Palpitations
- Edema (swelling) of the feet, ankles, or abdomen
- Rapid weight gain due to fluid retention.
What are the reasons and risks for heart valve repair or replacement surgery?
Valve repair or replacement surgery is performed to correct the problems caused by one or more diseased heart valves.
There may be other reasons for the child’s doctor to recommend heart valve repair or replacement surgery.
Possible risks associated with heart valve repair or replacement surgery include, but are not limited to, the following:
- Bleeding during or after the surgery
- Blood clots that can cause heart attack, stroke, or lung problems
- Infection at the incision site
- Pneumonia
- Breathing problems
- Arrhythmias (abnormal heart rhythms).
There may be other risks depending on the child’s specific medical condition. Be sure to discuss any concerns with his or her doctor prior to the procedure.
What happens before heart valve repair or replacement surgery?
- The doctor will explain the procedure and offer the patient and family the opportunity to ask questions about the surgery and what to expect afterward.
- The child’s primary caregiver (parent or legal guardian) will be asked to sign a consent form that gives permission for the procedure. It is important to read the form carefully and ask questions if something is not clear.
- In addition to a complete medical history, the doctor may perform a complete physical examination to ensure the child is in good health before undergoing the procedure. The child may also undergo blood tests or other diagnostic tests.
- The child will be asked to fast (not eat) prior to the procedure. Please see the CHOC NPO guidelines for more information.
- Notify the doctor if the child is sensitive to or are allergic to any medications, iodine, latex, tape or anesthetic agents (local and general).
- Notify the doctor of all medications (prescription and over-the-counter) and herbal supplements the child is taking.
- Notify the doctor if the child has a history of bleeding disorders or if the child is taking any anticoagulant (blood-thinning) medications, aspirin or other medications that affect blood clotting. It may be necessary for the child to stop some of these medications prior to the procedure.
- The doctor may request a blood test prior to the procedure to determine how long it takes the child’s blood to clot.
- Notify the doctor if the child has a pacemaker.
- Based on the child’s medical condition, the doctor may request other specific preparation.
What happens during heart valve repair or replacement surgery?
Heart valve repair or replacement surgery requires a stay in a hospital. The procedure may vary depending on the child’s condition. Generally, heart valve repair or replacement follows this process:
- The child will be asked to remove any jewelry or other objects that may interfere with the procedure and put on a gown to wear.
- The child will be asked to empty his or her bladder prior to the procedure.
- An intravenous (IV) line will be started in the child’s arm or hand.
- The child will be positioned on the operating table, lying on his or her back.
- The anesthesiologist will continuously monitor the child’s heart rate, blood pressure, breathing and blood oxygen level during the surgery. Once sedated, a breathing tube will be inserted through the child’s throat into the lungs and will be connected to a ventilator that will breathe for the child during the surgery.
- Additional catheters will be inserted in the child’s neck, top of the leg (groin) or wrist to monitor the status of his or her heart and blood pressure, as well as for obtaining blood samples. A catheter will be inserted into the child’s bladder to drain urine.
- The skin over the surgical site will be cleansed with an antiseptic solution.
- The doctor will make an incision (cut) down the center of the chest from just below the Adam’s apple to the end of the breastbone.
- The sternum (breastbone) will be divided in half with a special operating instrument. The doctor will separates the two halves of the breastbone and spread them apart to expose the heart.
- In order to perform the valve repair or replacement, the heart must be stopped to allow the doctor to perform the very delicate procedure. Tubes are inserted into the heart so that the blood can be pumped through the body by a cardiopulmonary bypass machine.
- Once the blood has been completely diverted into the bypass machine for pumping, the heart will be stopped by injecting it with a cold solution.
- When the heart has stopped, the doctor will perform the procedure by removing the diseased valve and putting in the artificial valve, in the case of a valve replacement. For a valve repair, the procedure performed will depend on the type of valve problem that exists, for example, separation of fused valve leaflets, repair of torn leaflets and/or the reshaping of valve parts to ensure better function.
- Once the procedure has been completed, the blood circulating through the bypass machine will be allowed to reenter the heart and the tubes to the machine removed.
- Temporary wires for pacing may be inserted onto the heart. These wires can be attached to a temporary pacemaker to help the heart rhythm, if needed, during the initial recovery period.
- The sternum will be rejoined and sewn together with small wires.
- The skin over the sternum will be sewn back together. The incision will be closed with sutures or surgical staples.
- Tubes will be inserted into the child’s chest to drain blood and other fluids from around the heart. These tubes will be connected to a suction device to drain fluids away from the heart.
- A tube will be inserted through the mouth or nose into the child’s stomach to drain stomach fluids.
- A bandage or dressing will be applied.
Learn what to expect the day of surgery at the Tidwell Procedure Center.
What happens after heart valve repair or replacement surgery?
In the hospital
After surgery the child will be taken to the cardiovascular intensive care unit (CVICU) to be closely monitored for several days. The child will be connected to monitors that will constantly display his or her electrocardiogram (ECG or EKG) tracing, blood pressure, other pressure readings, breathing rate and oxygen level. Heart valve repair or replacement surgery generally requires an in-hospital stay of several days or longer.
The child will most likely have a tube in his or her throat so that breathing can be assisted with a ventilator (breathing machine) until the child is stable enough to breathe on his or her own. As the child wakes up from the anesthesia more and starts to breathe independently, the breathing machine will be adjusted to allow the child to take over more of the breathing. When the child is awake enough to breathe completely by him or herself and is able to cough, the breathing tube will be removed. The stomach tube will also likely be removed at this time.
After the breathing tube is out, a nurse will assist the child to cough and take deep breaths every two hours. This will be uncomfortable due to soreness, but it is extremely important to do this in order to keep mucus from collecting in the lungs and possibly causing pneumonia.
Children experiencing pain are given pain medication. A nurse will show the child how to hug a pillow tightly against their chest while coughing to help ease the discomfort.
The child may be on special IV medicine to help his or her blood pressure and heart and to control any problems with bleeding. As the child’s condition stabilizes, these medicines will be gradually decreased and turn off.
The child may start drinking liquid once their breathing and stomach tubes have been removed and their condition has stabilized. The child will be able to eat solid foods as he or she can tolerate them. Gradually, the child’s activity will be increased, from sitting in a chair or wagon (as soon as breathing is stable on their own) to up walking in the hallway the day after surgery. Early activity is very important to prevent problems after surgery. The child’s care team will closely monitor the child to make sure his or her pain is well controlled.
When the child’s heart and breathing are completely stable, tubes have been removed, the child can take all medicines by mouth and the child is taking enough eating and drinking enough fluids and solids, the child’s care team will discuss going home. Arrangements will be made for a follow-up visit with the child’s doctor.
At home
Once at home, it will be important to keep the surgical area clean and dry. The doctor will provide specific bathing instructions. The sutures or surgical staples will be removed during a follow-up office visit, if they were not removed before leaving the hospital.
Notify the child’s physician to report any of the following:
- Fever and/or chills
- Redness, swelling, or bleeding or other drainage from the incision site
- Increase in pain around the incision site.
These instructions are for the purpose of general information and should not replace those provided by the child’s surgeon, nurses or other members of their health care team. Always contact the child’s doctor with questions and concerns.